|
This shows brain activity in the right temporal lobe before (to the left) and after (on the right) a chiropractic adjustment using Sacro-Occipital Technique (SOT®) which I practice in my office. The blue color indicates below normal brainwave activity as compared to a normative database and the red indicates above normal brainwave activity as compared to a normative database. Notice the absence of red color before the adjustment and the bursts of red color after the adjustment. Brain imaging is using BrainAvatar, Brainmaster Technologies, Inc. There's a first time for everything. And the neuroimaging above was a first!
The question "does chiropractic change the brain" has been the subject of 5 years of my research. Until my work, nobody had looked at live brain function and chiropractic. This video above shows the FIRST real-time imaging of what a brain looks like before and after a chiropractic adjustment. I had the exciting experiences of presenting this to others at Life University in 2014 and the Association of Chiropractic Collages Research Agenda Conference in 2015 as well as the Sherman college International Research and Phillosophy Symposium in 2015. How does this apply to patients? Let's say a person comes to me seeking help for headaches. We can look at the brain and see if there are areas that are abnormal. We can then see if those areas of the brain match the headache symptoms. We can then try interventions, for example chiropractic, and see if the brain is responding. If the brain is, then that's validation that what we are doing is helping (in addition to a person's report of symptoms, of course). If not, we can change what we are doing with a particular treatment or try something else entirely. Neurofeedback can be used for headaches. Metabolic testing and changes in diet and/or lifestyle may be what is needed to help a person. Or maybe the person is unhappy in their life and needs help in making a change. My job is to help people figure that out so that they can get better. I am excited to bring to my patients ground breaking technology and pioneering interventions. This is another part of what allows me to provide care to my patients unlike any other. This imaging was part of the firs three-armed randomized control study of chiropractic and brain function, which is coming soon to a major peer-reviewed journal near you.
1 Comment
 Attention-Deficit Hyperactivity Disorder (ADHD) is a condition that occurs in both children and adults. The Diagnostic and Statistical Manual of Mental Disorders 5th edition (DSM-V) defines ADHD by a collection of a certain number of symptoms. There are the inattentive symptoms (the attention deficit) and the hyperactivity/impulsivity symptoms (hyperactivity). Some of the more common complaints I hear from parents are that their child does not pay attention, does not seem to listen, is fidgety or is not performing well academically. But it is the consensus of the scientific community that true ADHD is a brain-based disorder. The vast majority of medical doctors, including psychiatrists, do not look at the underlying brain physiology when diagnosing ADHD and then prescribing medicine. To put that in perspective, imagine you had chest pain. Causes of chest pain are numerous. A short list includes myocardial infarction, coronary artery disease, myocarditis, pericarditis, pulmonary embolism, pneumothorax (collapsed lung), pleurisy, pneumonia, lung abscess, pulmonary hypertension, GERD (acid reflux), peptic ulcers, gallbladder problems, rib subluxation, shingles...and the list goes on. Imagine going to the medical doctor and having them tell you that they were not going to run any tests to figure out what was causing your chest pain. Instead, they were going to prescribe some medicine and see what happens. It seems ridiculous to even make up such a scenario, yet it is the standard of care with ADHD.  Using quantitative electroencephalography (qEEG) I can "look under the hood" with my patients and see what their brain is doing. The fascinating thing is that when that is done there is not one type of brain people with ADHD have. There are actually at least 6 different variants of brain activity that can result in the same symptom! And each variant responds differently to both Neurofeedback interventions and medications. Thus, ADHD is actually not one disorder. It is at least 6 different brain disorders presenting with the same symptom. Remember the chest pain example above?
It is not just me saying this. Published studies have been done on these different sub-types of ADHD and how they respond differently to medications, such as atomoxetine. Daniel Amen, a psychiatrist who is known for doing SPECT scans of people's brains, concurs that there are different types of ADHD brains that present with the same symptoms. He is now recommending Neurofeedback as a treatment for ADHD and other disorders. Patients who come to see me for ADHD will get a qEEG evaluation done to assess brain function. They will also get computerized testing done to confirm that they actually have ADHD and help determine that they do not, in fact, have another disorder that has some of the same symptoms as ADHD. Sometimes, when I run the tests for ADHD, I discover that the person who was being prescribed medication for ADHD does not even have this disorder. People can have other problems that mimic ADHD including Autism Spectrum Disorders, sensory integration problems (often but not always related to autism), auditory and/or visual processing disorders, developmental trauma or Oppositional Defiant Disorder. I also utilize a program called Brain Dx which is a qEEG normative database developed over decades of peer-reviewed, published research at New York University. Brain Dx has a discriminant function that tells the doctor the likelihood that a brain is one of a person having ADHD. Discriminant functions in neuroimaging are not stand alone instruments for diagnosis. However, in conjunction with other testing and assessment measures, they can offer valuable insight into the organic basis of psychological problems. There are also discriminants for things like major depression, bipolar disorder, schizophrenia, dementia, autism and traumatic brain injury. I use whichever ones are appropriate when working with patients. I have had excellent success treating ADHD. While working at the Psychological Sciences Institute, I worked with a neuropsychologist and we presented our research on ADHD at the International Pharmaco-EEG conference in New York City. In our sample of 41 people, 100% of subjects had improvement in their attention and impulsivity scores using the IVA+ continuous performance test (objective computerized test) after Neurofeedback treatment. YES, 100%. Here is a link to the poster we presented. ipeg_poster_2012_final-1.pdf. Publication of this material is in development. At the end of this blog is a list of over 100 more studies on Neurofeedback and ADHD. There are a handful of studies on chiropractic and ADHD. Most are case studies and present very limited objective evidence. However, in certain cases I have seen chiropractic be an effective intervention. I am able to provide chiropractic as a stand-alone trial intervention or in conjunction with other therapies should a patient request such. My goal is to help people get better as soon as they can. Another co-factor of ADHD can be metabolic dysfunction. This can often relate to things like gut dysbiosis with associated food sensitivities. Poor diet will facilitate such a condition and perpetuate it. Other more complex metabolic processes and neuro-inflammation can be at play and I can test for these at my office. If you or a loved one struggles with ADHD, or you think they might have ADHD, please contact me to set up a consult and evaluation. It would be an honor to help you. Here is a list of over 100 studies on Neurofeedback and ADHD, cognition and learning disorders: Click here: Over 100 ADHD studies 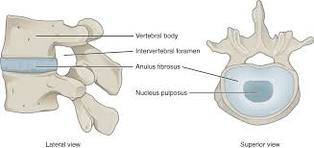 By OpenStax College [CC BY 3.0 http://creativecommons.org/licenses/by/3.0)], via Wikimedia Commons By OpenStax College [CC BY 3.0 http://creativecommons.org/licenses/by/3.0)], via Wikimedia Commons Low back pain? Leg pain? Sciatica? Often we have come to think of that as a disc problem. Your spine is made of vertebrae stacked on top of each other. Sandwiched in between the vertebra is the intervertebral disc. Discs are like padding between the vertebra. When a disc ruptures, its jelly-like contents can spill, irritating nerve roots and causing pain. Discs became popular as the culprits of low back pain when MRI's came out and you could really see the discs. But here's the catch: there are a lot of abnormal MRI's with unhappy looking discs and the people have no low back pain at all! . Turns out that discs aren't the cause of a majority of low back pain cases. What has been overlooked for a long time by the medical field is the sacroiliac joint. Chiropractors have been talking about it since the 1920's. And medicine is now catching on. Sacro-who? The sacrum is the bone at the base of the spine. It's the one people call their tailbone, although technically the tailbone is the coccyx which is one segment lower. The sacrum attaches to your hip bone to form the sacroiliac joint and your pelvis. 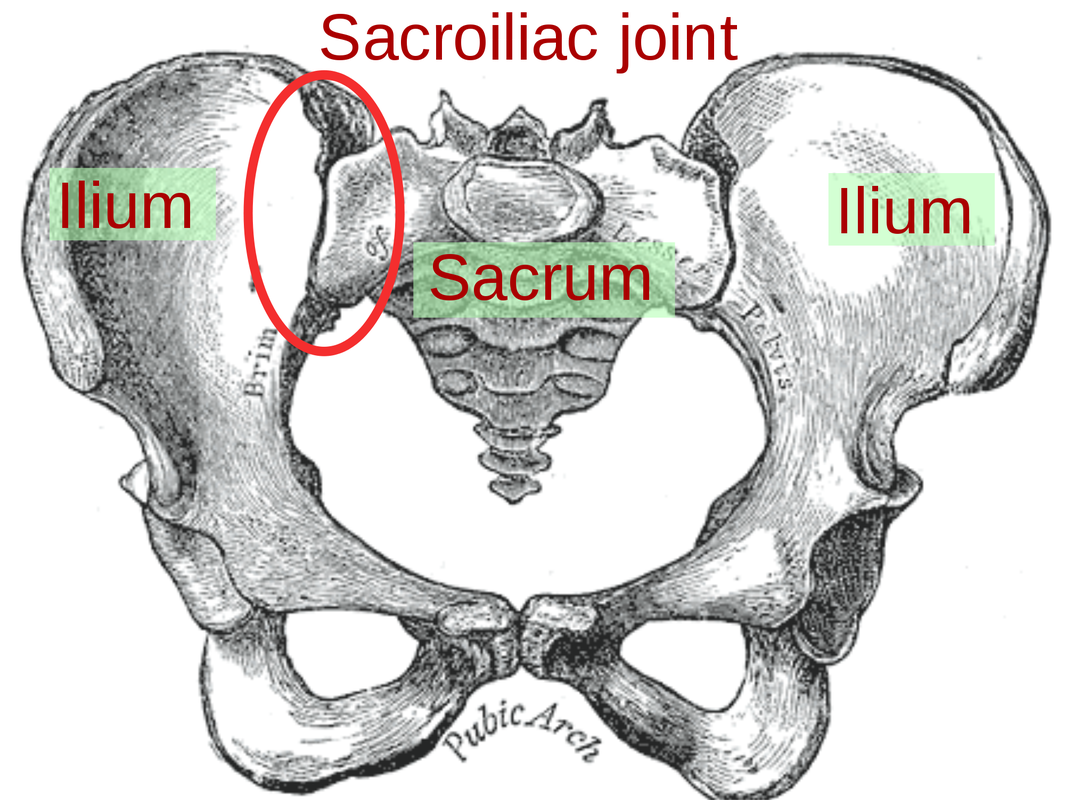 By Mikael Häggström (File:Gray242.png) [CC0], via Wikimedia Commons  By Ldpedersen (Own work) [GFDL (http://www.gnu.org/copyleft/fdl.html), CC-BY-SA-3.0 (http://creativecommons.org/licenses/by-sa/3.0/) or FAL], via Wikimedia Commons By Ldpedersen (Own work) [GFDL (http://www.gnu.org/copyleft/fdl.html), CC-BY-SA-3.0 (http://creativecommons.org/licenses/by-sa/3.0/) or FAL], via Wikimedia Commons Here's some random trivia: The word sacrum derived from the Latin word Sacer meaning sacred. The sacrum in Latin was os sacrum meaning "holy bone." The holiness of the bone is up for debate, but its importance is not - it's really important!
The sacroiliac joint has had some controversy. Chiropractors said it moved. Medical doctors said it was immobile. And everyone argued over it. It's accepted now that portions of it do move. The sacroiliac joint forms the foundation of the spine. Think of the foundation of your house. A house with a solid foundation will be solid. A house on a cliff with a bad foundation will be in all sorts of trouble. And so will your spine if if it doesn't have a properly functioning sacroiliac joint. The sacroiliac joint has multiple functions. In part 1 of the sacroiliac joint blog, I'm going to talk about the weight bearing part. Weight bearing means joints and those that respond to things like standing. The sacroiliac joint has a weight bearing part. Other weight bearing joints include your hips, knees, your ankles. The weight bearing part of the sacroiliac joint should not move (another part should move - see part 2 of this series). The weight bearing portion of the sacroiliac joint held together by strong ligaments. Problem is, these ligaments can become stretched and the part of the sacroiliac joint that shouldn't be moving starts moving. This creates instability in the pelvis --- and everything resting on top of that pelvis gets disrupted too (remember the house with the bad foundation?). The muscles of the low back and pelvis respond, tightening in an attempt to stabilize things. And there is your low back pain. It's really quite simple in these instances --- if you stabilize the sacroiliac joint, the muscles will quiet down and suddenly there isn't pain anymore. Although if the problem has been there for 10 or 20 years, the muscles will need some work too. But what else is above the pelvis? How about the shoulder. Many shoulder problems are actually reactions to pelvis problems. I had a patient in my office the other day complaining of not being able to raise their arm (frozen shoulder). I corrected the sacroiliac joint and the person was suddenly able to lift their arm. I never even touched their shoulder! What connects to the shoulder? How about the elbows and wrists. And you guessed it, elbow and wrist problems can be the result of a sacroiliac joint problem. Wild, isn't it? It gets even more crazy though. The neck sits on top of the shoulders. Yep, neck pain can be the result of a sacroiliac joint problem. What's on top of the neck? The head, of course. Tempromandibular joint (TMJ) problems or jaw problems can be (and always are related to) sacroiliac joint problems. By now I should have rocked your world. Let me rock it a little more. What about the other weight-bearing structures: remember, the hips, knees and ankles. Well they are also affected by the sacroiliac joint. Knee pain, ankle pain, foot pain, hip pain - they all can be caused by an unstable sacroiliac joint. Similarly, problems in the knees, ankles, hips, and feet can cause sacroiliac problems, but that's for another blog entry. I specialize in sacroiliac joints and love to fix them. And I mean that, I really am passionate about it. I had a patient who had been to 4 other chiropractors, a physical therapist and a pain management clinic for low back pain with minimal results. The problem was they were treating her disc and the problem was, you guessed it, her sacroiliac joint. One adjustment and she was feeling much better. Watch out for part 2 of the series on the sacroiliac joint - the part that is supposed to move. |
AuthorI'm a Chiropractic Physician, Psychotherapist and researcher. I'm interested in helping people live their lives to their full potential. That could be simply without pain. Or it could be without more complicated physical or mental health problems. Or it could be getting help in making changes in their life so that they can achieve their dreams. Archives
June 2023
Categories |
 RSS Feed
RSS Feed